

By Alex Ababio
Born With Symptoms, Still Undiagnosed
The afternoon heat in New Tafo Krofrom, a crowded inner-city community in Kumasi, was intense. The air barely moved, and sweat gathered easily on the skin. Inside a dim, poorly ventilated room, Rita Fosua sat on the edge of a thin, worn mattress.
The roof leaks when it rains. The floor is cracked and full of holes. Insects crawl along the walls. This is where she lives with her four children.
In her arms lies Kwaku — one and a half years old — his head bent backward at an unnatural angle, his tiny ribs visible beneath fragile skin. He has never sat on his own. He cannot look straight; his eyes drift sideways. Since birth, he has never suckled his mother’s breast.
“My son was born at Old Tafo Government Hospital,” Rita Fodua recalls, her voice steady but tired. “Right from birth he did not cry. His eyes were closed and he couldn’t open them. The doctors put him in a machine for a long time. They could not figure out what was wrong.”
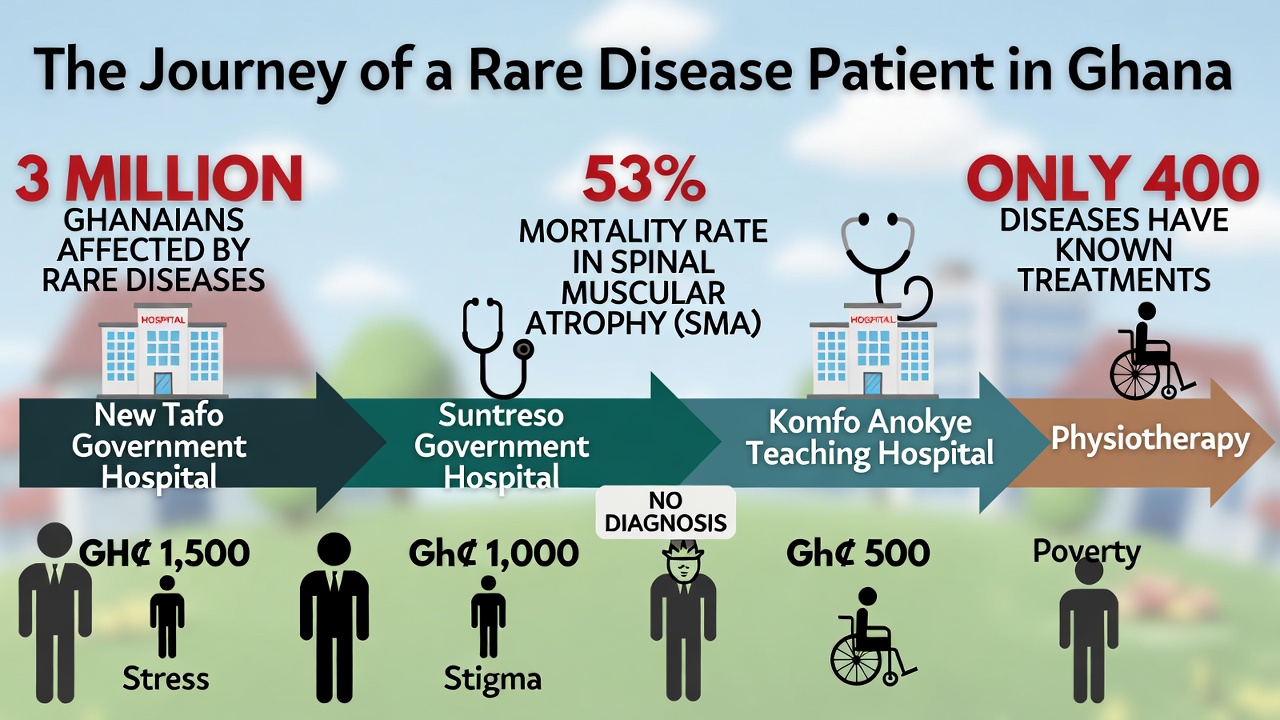
From old Tafo Government Hospital to South Suntreso Government Hospital. From there to Komfo Anokye Teaching Hospital. At each stop, the same question echoed: What is wrong with this child?
No Doctor Could Name His Illness :
At Komfo Anokye, Kwaku finally opened his eyes — but he still could not fix his gaze. Doctors issued internal referrals. They asked for physiotherapy. They ordered checks on his eyes, ears and cognitive function. Rita and her husband managed two physiotherapy visits at Manhyia Government Hospital in Kumasi. Each visit cost GH¢100.
And That’s When the Family Hit Empty Pockets
The father, who survives on irregular menial jobs, has spent more than GH¢10,000 since Kwaku was born. The family now buys canned food because Kwaku cannot breastfeed. Some days, they cannot afford even that.
“We don’t know how much they will charge to check his mind, eyes and ears,” Rita says. “We have no money again.”
They turned briefly to herbal medicine when orthodox treatment brought no answers. It was even more expensive. They stopped.
Now Kwaku lies quietly in the dark room that smells of dampness and exhaustion — a child without a diagnosis, a family without hope.
Kwaku’s Story Reflects the Plight of Millions of Unseen Ghanaians.
In Ghana, millions of children like Kwaku are trapped in a diagnostic desert — rooms full of uncertainty, tests that don’t exist locally, and doctors struggling with conditions they can’t name.
American geneticist and bioethicist Dr. Charmaine Royal emphasizes : The global imbalance in genetic data not only undermines equity in diagnosis but also limits the development of treatments for underrepresented populations,” highlighting why the lack of local data has devastating consequences.
A Hidden Population, Hurting: Three Million Forgotten Ghanaians Living with Rare Disease
In Ghana, an estimated three million people — roughly 10% of the Ghana’s 35.5 million population — are living with rare diseases,
According to Professor Jerry John Kponyo, Scientific Director and Project Lead of the Responsible Artificial Intelligence Lab (RAIL) at the Kwame Nkrumah University of Science and Technology Engineering Education Project,
Professor Jerry John Kponyo
Globally, more than 350 million people live with rare diseases, according to the France-based Fondation Ipsen. The U.S.-based National Organization for Rare Disorders estimates that 30 million Americans — also about 10% of the population — are affected. Around 95% of rare diseases have no approved treatment.
Yet in Ghana, the challenge is compounded by a severe diagnostic gap.
Professor Kponyo explains that
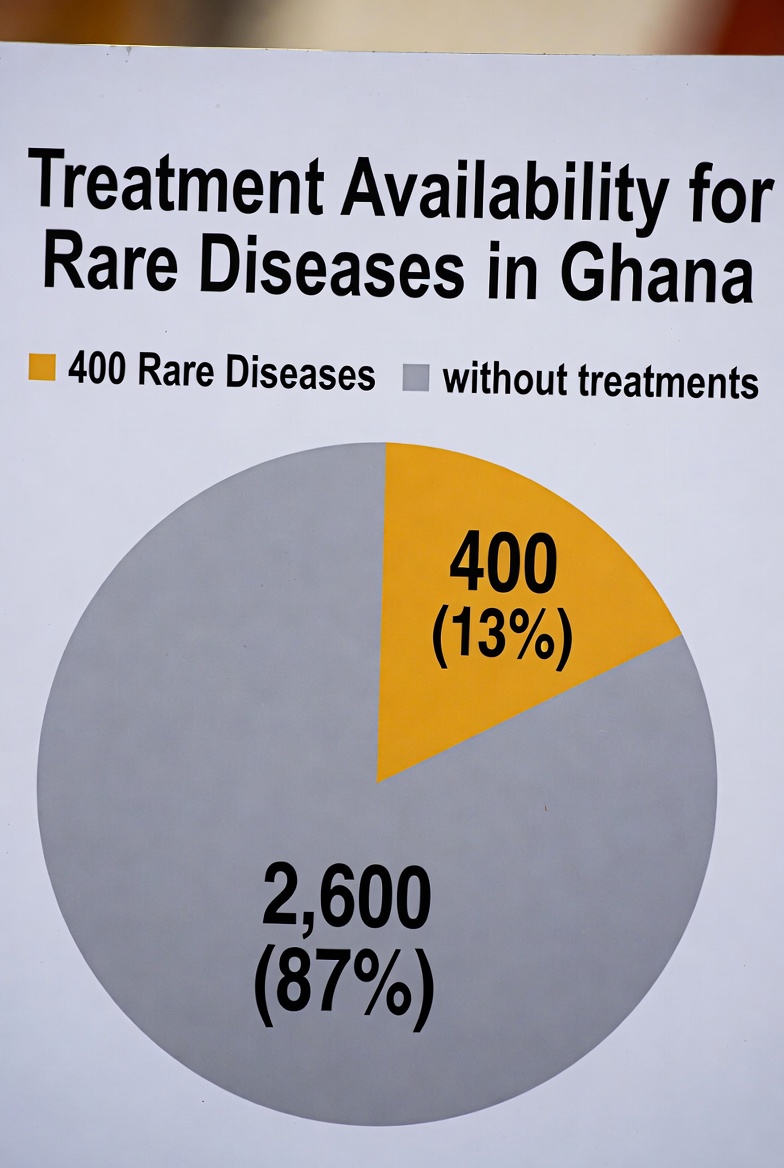
between 6,000 and 8,000 rare diseases have been identified globally. Only around 400 have treatment plans — and many of those depend on precise genetic understanding.
“One thing about rare conditions,” he says, “is that they are often caused by a single gene. If you can identify that gene, you can tailor treatment.”
But identifying that gene requires genetic testing — a service that can cost up to $10,000 per family.
How many Ghanaian families have $10,000 sitting idle? Certainly not Rita.
No Name, No Hope: The Diagnostic Gap :
The Executive Director of Rare Diseases Ghana Initiative, Samuel Adjei Wiafi, does not mince words.
“The biggest issue is that there isn’t a policy. There’s no clear national plan for rare disease patients,” he says. “The diagnostic infrastructure is woefully inadequate.”

Through a philanthropic diagnostic access program, his organization has supported nearly 400 families with genetic testing — at roughly $10,000 per test. Multiply that.
That is nearly $4 million raised largely through philanthropy, not government systems.
“It’s not sustainable,” Wiafi admits. “If a patient is suspected anywhere in the country, they should be able to get testing done affordably, ideally covered by insurance.”
But Ghana’s National Health Insurance Scheme (NHIS) reimburses based on coding systems. Many rare diseases lack proper coding integration. Even though the global ICD-11 classification includes many rare diseases, it remains unclear whether full integration into Ghana’s reimbursement structure has occurred.
NHIS Ashanti Regional Director Muniru Mohammed Muntaka argues that about 95% of diseases and medications are covered. He points to the Ghana Medical Trust Fund — popularly known as Mahama Care — as an initiative to support conditions not covered.
“The scheme must be sustainable,” he explains. “If we bring in all cancers and rare diseases at once, it could collapse the scheme.”

He emphasizes actuarial projections and financial stability. The government, he says, is building capacity gradually.
For families like Rita’s, gradual feels like never.
Children Dying Before Diagnosis
Spinal Muscular Atrophy (SMA) offers a window into the crisis.
Between 2018 and 2023, 17 SMA cases were confirmed across five centers in Ghana, according to hospital records cited by Dr. Charles Kumi Hammond,
Associate Professor, Department of Child Health, KNUST & Consultant Pediatric Neurologist, Komfo Anokye Teaching Hospital KATH, Kumasi
Nine of the 17 children — 53% — died.
Four had originally been referred as cerebral palsy. Four were labeled broadly as neuromuscular disorders.
Five families paid for overseas genetic testing. Twelve relied on special programs.
Globally, SMA incidence ranges from 1 in 6,000 to 1 in 10,000 births. In the United States, prevalence is about 1 in 10,000 individuals. In Ghana, prevalence is unknown — largely because newborn screening does not exist.
Management here remains supportive: physiotherapy, respiratory care, genetic counseling. The life-saving gene therapies available elsewhere are not accessible.
One surviving Ghanaian child with SMA type I received newborn screening overseas and gene therapy. That child lives.Others did not.

The Eye Cancer That Steals Sight
Dr. Samuel Tenagyei, a leading optometrist in Kumasi, speaks about retinoblastoma — a rare childhood eye cancer affecting children under five.
“The symptoms are classical,” he says. “It is not difficult to diagnose. But it is difficult to manage.”
Prognosis is often poor. Saving vision — sometimes even life — becomes uncertain.
He highlights systemic weaknesses: limited state-of-the-art equipment, inadequate genetic testing, insufficient data systems.
“Most of the time it goes undiagnosed or is labeled cause unknown,” he says.

He describes the psychological trauma of families shuttling from one hospital to another, enduring trial-and-error treatments. “Imagine the anxiety, the fear, the loss of hope,” he says. “And of course, in our setting, we quickly resort to spiritual explanations.”
In the absence of diagnosis, superstition fills the vacuum.
Stigma, Silence, and the Weight of Spiritual Blame :
Elizabeth Emmanuella Nimon, National Secretary of the Ghana Society of the Physically Disabled, describes a 12-year-old boy in Bekwai. The child suffers mysterious symptoms — mouth sores that migrate, sensations of intestines “folding,” constant hospital visits without answers.
“Every time they go, they are told a different thing,” she says. “They are not able to get specific treatment.”

Families are accused of witchcraft. Children are whispered about. Mothers are blamed.
Neurofibromatosis patients with facial tumors struggle to attend school or church without ridicule. Down syndrome children with congenital heart defects require surgeries families cannot afford.
Wiafi puts it bluntly: “The moment they have a child with a rare disease, they start moving toward the poverty line.”
Kwaku’s family is already there.
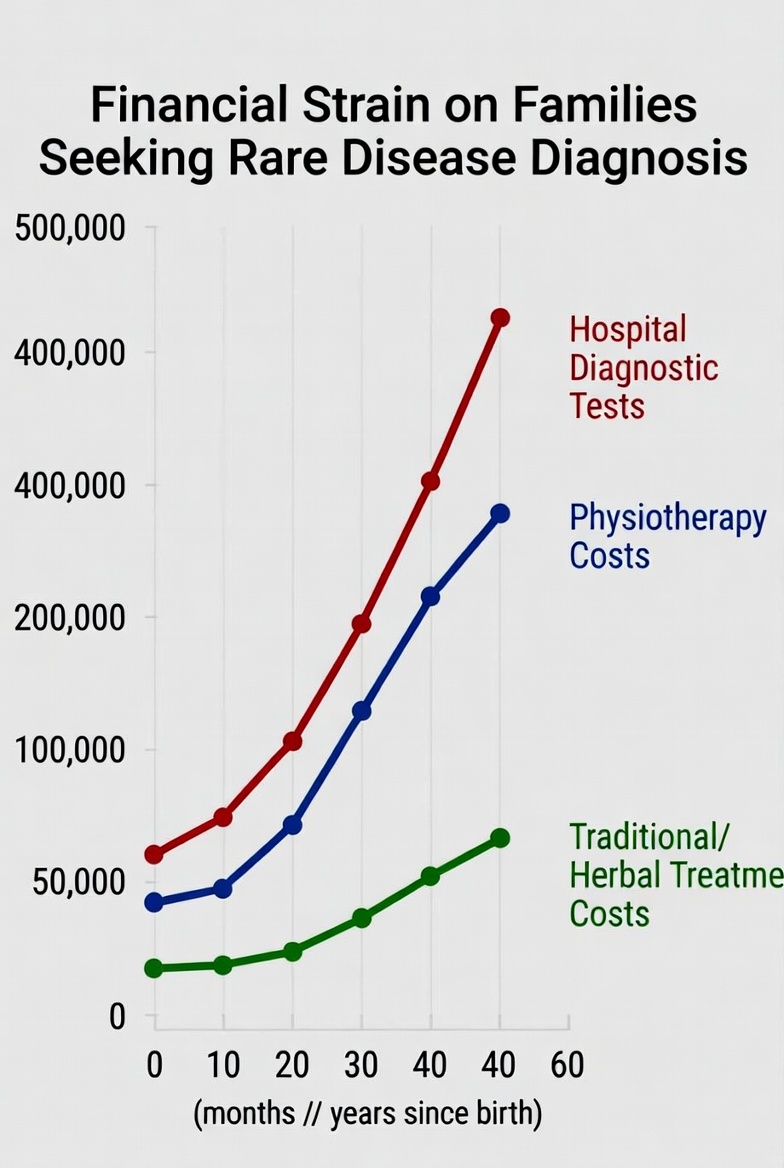
Who Profits, Who Suffers: Following the Money
Rare disease care is expensive everywhere. But in high-income countries, insurance systems, social safety nets and research funding cushion the blow.
In Ghana, families pay out-of-pocket.
Physiotherapy: GH¢100 per session.
Genetic testing: up to $10,000.
Cochlear implants: tens of thousands of cedis.
Congenital heart surgeries: unaffordable for most.
NHIS may cover consultations and some labs, but advanced diagnostics, genetic tests, assistive devices and orphan drugs often fall outside reimbursement structures.
Childhood cancers were recently considered for inclusion. That is progress. But thousands of other rare conditions remain uncovered.
The financial burden pushes families downward — sometimes permanently.
A Global Mandate — Will Ghana Act?
On 24 May 2025, the World Health Assembly unanimously adopted a Resolution on Rare Diseases. It recognizes rare diseases as a global health priority and calls for improved diagnosis, treatment, care and research.
Ghana co-sponsored the resolution.
The resolution requests a 10-year Global Action Plan.
The world has spoken.
Will Ghana listen to itself?
Artificial Intelligence and a Flicker of Hope
At KNUST’s Responsible AI Lab, researchers are building tools to analyze genomic data at scale. Their model compares patient genetic information with a global pool of 29 million shared datasets.
In one case, a woman lost four babies shortly after each birth. Doctors treated recurrent convulsions without identifying the root cause. The KNUST Engineering Education Project -RAIL Genetic analysis revealed a condition triggered by breastfeeding. When she avoided breastfeeding with her next child, the baby survived.
From Numbers to Hope: How Data Saved a Life
But hope is emerging. Pilot programs using genomic data have already changed outcomes for some children, turning numbers into lifesaving interventions.
“Professor Shahida Moosa, a leading genomic clinician in South Africa, says building diagnostic capacity tailored to African genomes is essential — not optional — if millions are to be diagnosed accurately and early,” signaling that with proper investment, the story of Kwaku could be replicated for thousands more.
The Scientific Director and Project Lead of RAIL Professor Kponyo believes Ghana can lead Africa by integrating AI-driven genomic tools into public health systems.
But algorithms cannot function without data. Data cannot exist without testing. Testing cannot happen without funding and policy.
“At the Responsible Artificial Intelligence Lab, our main goal is to ensure that the innovative solutions we develop actually reach and benefit people. There’s no point in creating a solution if it’s never used. That’s why, with our Care for Rare Disease program, we aim to partner with the Ministry of Health and the Ghana Health Service to address challenges related to rare diseases.” , Professor Kponyo explained
Technology alone cannot fix systemic neglect..What Must Change
Experts agree on several urgent priorities:
A comprehensive national rare disease policy.
Integration of rare diseases into NHIS coding and reimbursement.
Investment in genetic testing and newborn screening.
Expansion of specialist services — physiotherapy, speech therapy, occupational therapy.
Inclusion of orphan drugs and assistive devices on the essential medicines list.
Incentives for research and data management.
Public awareness campaigns to reduce stigma.
Rare Diseases Ghana Initiative is engaging policymakers. Advocacy forums have been held with the Ministry of Health.
But policy drafts do not breathe for children like Kwaku.
Trapped in the Dark: Life in a Forgotten Room :
As evening falls in New Tafo Krofrom, Rita adjusts Kwaku’s head gently so he can breathe comfortably.
She does not know the name of her son’s condition.
She does not know whether he will sit, speak, or survive.
She only knows that she has walked from hospital to hospital, from hope to hope, spending money she did not have.
Three million Ghanaians live in similar uncertainty — invisible in statistics, absent in policy, waiting in dark rooms across the country.
Rare but deadly.
The question is no longer whether Ghana can afford to prioritize rare diseases.
It is whether Ghana can afford not to.
Because every day without diagnosis is not just a policy delay.
It is a childhood slipping away.
This story was published with support from the US National Press Foundation